
Weight on the boad 2511.
Nurse today is a primary, we are glad to see her.
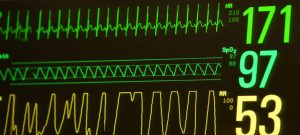
23% oxygen CPAP weaned to 6. That’s awesome!
She tells us about a massive poop he had earlier that got messy. I’m kind of jealous that I wasnt there. It is officially his first blow out, had to change his clothes and bedding!
Proud of him for pooping so well lately considering the toll the extra fortification we put in his milk. It’s impressive he has done as well as he has.
He had a pretty good night too! 5 events, almost all self corrected. Mostly not deep either. Good job buddy!
1050 Large event, preceded by a cough. Presents itself as potentially a bronchial spasm triggered by the cough. Was the cough caused by rainout? He requires stim to come back up.
Heart rate into the 60’s, spo2 into the 40’s.
After the event he looks fine. Obviously his mom and I are stressed and searching for answers.
His albuterol was dis continued yesterday… was it helping. Was it a true bronchial spasm?
When a baby has a bronchial Spasm it also looks like apnea because they can’t breathe so respiration rate goes down.
So is it just not wanting to breathe after rainout or a painful cough?
Or is it apnea because his Theofalin level has not been checked in over a week?
Apnea also causes a brady event.
After the event weaned to 24%
Cares, 36.6. Just pee. Binky time.
Then two more major events similar to the other. One preceded by a cough, the other one not.
One event has more than a full page of apnea and drops to 60 spo2 before the nurse is able to react or come assist, low spo2 into the 30’s
I ask if it is better to catch him before he falls so low or to let him drop. Am I allowed to stim to get him to breathe before the nurse arrives?
Nurse says even though it’s hard to tell me this and it is hard to hear and do, I am not allowed to, they want to let him do his thing so that they can see what is happening and gather accurate information and be the one to do the stim and see what is required and accurately describe to the doctor what was needed .
While I agree that it is important to see what is happening, we are gaining no information just by letting him fall lower, other than seeing if he can self correct at a certain point it becomes apparent that he wont..
I only have a tolerance to let him drop to a certain point before I feel it is complete negligence for me to sit and wait for someone else to do something.
If he has a full page of apnea I already know he is going to drop his spo2 into the 40’s or lower. The deeper he goes the worse it is for his development brain and all organs, under 80 spo2 and all organs are beginning to be oxygen starved, and the longer it will take for him to recover.
Have you ever been to 15,000 ft? Your spo2 will be about 80. Doesn’t feel good, spo2 of 65, that is like being at 20,000 ft.
While other babies with less chronic lungs may have an episode of not breathing, once they get pressure and some breathes on the neopuff they would be able to come up quickly because they are able to oxygenate their blood efficiently.
For RT it is more difficult with many factors working against him like damaged lungs that don’t work too efficiently.
While I agree it is important for the trained nurses to get the full picture, see trends, see if changes to meds, weaning of settings or an indication of being sick or seeing if he can self recover on smaller events and try and make observations about what is required to get him back up and have a thesis about the what caused it.
I am the one sitting there observing what the potential causes are, the length of time before the system even decides to alarm while he drops quick, how fast he is falling, I have a pretty good idea of how deep he will go because of how long he had not already been breathing, we sit there studying him and his monitors, analyzing everything for 12 to 15 hours per day for the last 88 days.
At a certain point he is obviously not going to self correct and the issue then becomes how do you make him recover.
When does the damage then begin to start weighing heavier than the gain.
It is damaging to his health to let him continue to have these larger events.
It is extremely frustrating to just be required to sit on my hands while my son changes colors and visibly requires assistance….
When he is angry with a high heart rate they encourage me to help calm him down with patting, hand hugs, binkys, milk swabs. They don’t want him angry because it causes other issues like, weight loss.
But if he has a low heart rate and is nearing being unconscious with a low spo2 causing brain damage and developmental issues I’m asked to sit and wait till help arrives.
Nope I can’t do light stim to get him to come back up even if he has extreme hypoxia.
Extreme hypoxia (SpO2 <40%)
The effects described above are those of severe hypoxia. Progression of the severity of hypoxia finally results in extreme hypoxia. Extreme hypoxia eventually causes failure of brain stem functions. The brainstem is a part of the brain most resistant to the effects of hypoxia, and only malfunctions and fails at degrees of hypoxia causing failure of the rest of the brain. Extreme hypoxia causes failure of all cerebral cortex functions, as well as brainstem malfunction so inducing loss of consciousness, together with abnormal breathing. Even more extreme hypoxia causes failure of all brainstem functions, causing loss of consciousness and cessation of breathing, resulting in anoxia, subsequent irreversible brainstem damage and death.
There is somewhere a disconnect, because I know this is not the nurses decision that I do this.
I’m not mad at the nurse she does an excellent job, it’s just a bad stance of the medical world and probably some parents would even stim when he hit’s an spo2 of 80.
I’ll tell you what though, if he needs it the nurse will get an accurate description of how low he was, what he needed and how long it took.
Don’t know why I even asked the question, the answer was what I expected but more frustration than expected.
Lunch time.
He has been having these types of events on and off essentially since his eye surgery. No known correlation that I have seen between medications helping it between his albuterol or variant, caffeine, or Theofalin. Some nights many more events, some nights almost none.
Over lunch I essentially come to the decision he is not having bronchial spasms.
If he was, then stim would not cause him to breathe again, he wound only start to breathe once the spasm subsided…
He has not had an apnea issue in the past, the first time his Theofalin was discontinued it was because the level was too that it was not helping him anyways. Swapped to caffeine because it is easier to keep in therapeutic range. No difference in events, swapped back to Theofalin because they had to try something.
Nether seems to really have much of a change on his events.
I don’t think it’s him forgetting to breathe and going apnic.
I come to the decision and convince myself it is almost all related to rainout.
Condensation in his ventilator tubing increases as the temperature of the room decreases cooling the air as it flows through the tubing. Warm air holds more moisture, it condenses as it cools off, creating droplets that eventually get forced into RTs nostrils by way of 10 liters per minute of airflow going past his nostrils.
Slug of water could prompt the coughing, the occasional random anger, not wanting to breathe or locking up. Not exactly traditional apnea. More of the description of reflex Apnea
The premature infant also manifests an immature response to peripheral vagal stimulation. For example, stimulation of laryngeal receptors in the adult results in coughing. However, stimulation of these same receptors in the premature infant results in apnea. This reflex apnea can be induced by gavage feeds, aggressive pharyngeal suctioning and gastroesophageal reflux.
I imagine water flying down the airways causes the same effect. He is also bradying. I imagine when he coughs it could make him not want to breathe too just from secretions or a painful cough.
Bradycardia by itself is often a sign of obstructive apnea. No apnea alarm is sounded because the chest wall is moving even though air flow is absent. Also reflex apnea can lead to bradycardia within 2 seconds of onset, thus setting off the cardiac alarm 10 to 15 seconds ahead of the apnea alarm.
Back up to do cares. Nurse tells us he had another large event, doctor started back up the albuterol in hopes that it will stop the events thinking that because they are prompted by a cough is bronchial spasms.
Well sure it’s worth a try, while I don’t think it has helped in the past.
1400 we do cares, I decide no skin to skin today he has had a rough day. He needs some rest. Albuterol is in.
After a discussion about rainout the respiratory therapist gets a new piece that goes to his nose that builds up water quick, within minutes it is dripping water again. She is surprised it happened so fast. I explain that’s why I’ve been trying to keep it covered with a wash cloth, she agrees, they have tried blankets over them in the past. She gets all new tubing and humidifier dome, then tries covering most of the tubing with blankets. It appears to help the rainout build up slower.
We decide to go on a walk, grab hot coffee.
Head back after a while. No events while we were gone.
1700 Cares, still no events, almost no condensation in the tubing. Is it just a time he had no events, would have had no events anyways or is less condensation helping, or is it the albuterol stopping bronchial spasms?
Dinner.
Shift change.
Another large event.
Next albuterol dose started early.
New nurse that has never had him.
Respiratory therapist tonight doesn’t like the way the blankets are too close to the heater for the humidifier so she does it her own way. Immediately there are larger fluctuations in the humidifier temperature. Hopefully this doesn’t cause more rainout. Everyone has their own way of trying to help.
2000 Cares he poops as I’m about to change his diaper! Glad he got it out first this time. Maybe working on that caused this last event who knows. Swaddled up.
Within 15 minutes another large event. Last night no big events like this and not on albuterol. He Is back on it and has still having the same type of event. I don’t think it’s helping much.
Well at least he is still recovering from events quick.
If we can keep weaning his setting maybe move to vapotherm which tends to have less rainout!
Long and stressful day but. except for the events…. He had a pretty good ok day. Although I feel like this could be said most days…maybe it just wasn’t a bad day.
Please have a good night morning my boy.
Morning because it is already 0244. Time for bed.
